| Home | Vein of Galen Malformations | About Anna | Pictures | Memorial Funds | Links & Contacts |
| This is a very rare condition affecting the blood vessels of the brain. The
abnormality occurs during embryonic development and results in abnormal communications
between the arteries and the veins in the blood vessels of the developing brain. The
capillaries which normally connect arteries to veins and function to slow blood flow
allowing for the drop off of oxygen and nutrients to the brain are missing. Since vein
of Galen malformations lack capillaries, blood flow can be fast and this in turn
increases the work of the heart. Blood drainage is towards a single deep draining vein,
which becomes markedly enlarged (vein of Galen aneurysm). The result can be heart
failure. The high flow of blood can also interfere with the normal blood drainage of
the brain potentially causing hydrocephalus or 'water on the brain'. This rare
malformation develops in utero. These patients may be newborns with congestive heart
failure due to arterial-venous shunting of blood in the brain.
Sometimes this abnormality can be detected during an antenatal ultrasound scan, but not always. In particularly severe cases, the growing baby has difficulty coping with this abnormal shunt and it develops heart failure. Sometimes this is so severe that the baby will die in utero. Often this is not the case and the baby is born, but rapidly goes into heart failure after birth. Sometimes this can be managed medically until the baby is a bit bigger, but sometimes the baby has to be treated in the neonatal period. Sometimes the heart failure is so severe that it affects all the other organs, including the lungs, liver, kidneys and brain and then despite treatment the baby will not survive. If the baby has only mild heart failure it is safer to try and grow the baby until it is a little easier to treat. Other children with vein of Galen malformations never develop heart failure, but because of the abnormal communications between the arteries and veins, the water that is inside the head and brain cannot be properly absorbed. This leads to an accumulation of water within the baby's head, so that the baby starts to develop a very large head. Often these babies are a little bit 'floppy' and sometimes just a little developmentally delayed. These children can be treated at a few months of age. Their heads often remain large, but they 'grow into' their head size over time. Following embolization these children often make rapid steps forward in their development. Children in whom the diagnosis is missed or remains untreated are at risk of developing permanent brain damage. The abnormal communications affect the ability of the blood vessels to mature properly and can result in a permanent high pressure within the blood vessels. This affects the brain tissue, which fails to grow properly and can malfunction. These children may develop seizures or fits and may develop symptoms of a stroke.
Angiogram and MRI of a Vein of Galen Aneurysm. Anna's Vein of Galen was the diamter of a quarter. Her 4 embolization procedures required 90+ platinum coils. Picture of AVM blood flow (Flash required) |
||||||||||||
| Endovascular Therapy
Endovascular treatment uses small catheters inserted into your blood vessels to deliver glue or other obstructive materials into the AVM so that blood no longer flows through the malformation. It is performed in the angiography suites of the Radiology Department by a Neuro Interventionalist. The procedure is performed under general anesthesia. A small incision is made in the groin and a catheter is inserted into an artery then passed through the blood vessels to the feeding arteries of the AVM. Occluding material, either coil or acrylic glue, is passed through the catheter into the AVM. The procedure time can vary, and the patient remains in the hospital several days for observation. The advantage of this treatment is it’s less invasive than surgery and can be used to treat deep or inoperable AVMs. Disadvantages include risk of embolic stroke from the catheter and rebleeding since the AVM is not completely obliterated. Often a patient will require more than one embolization. Some patients may be cured by partial embolization. Many patients grow up completely normal after treatment. The risk of treatment varies but may be as high as 10% for permanent disabling stroke or death. |
||||||||||||
|
||||||||||||
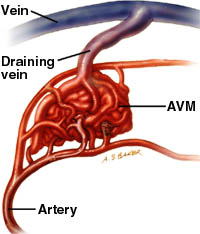
| What is an ArterioVenous Malformation (AVM)?
Normally blood flows from the heart through large arteries to all areas of the body. The arteries branch and get smaller until they become a capillary, which is just a single cell thick. The capillary bed is where the blood exchanges oxygen and nutrients with the body tissues and picks up waste. The blood travels from the capillary bed back to the heart through veins. In an AVM, arteries connect directly to veins without a capillary bed in between. This creates a problem called a high-pressure shunt or fistula. Veins are not able to handle the pressure of the blood coming directly from the arteries. The veins stretch and enlarge as they try to accept the extra blood. The weakened blood vessels can rupture and bleed and are also more likely to develop aneurysms. The surrounding normal tissues may be damaged as the AVM “steals” blood from those areas (arrowhead). |
||||||||||||
|
||||||||||||
| Angiogram depicts a large AVM in the parietal lobe of the brain. Feeding arteries lead to a tangled nidus (arrow) that shunts blood directly into a large draining vein. | ||||||||||||
|
||||||||||||
| Platinum Micro-Coil Treatment for Aneurysms
Micro-coil is a soft, platinum coil that is attached to a stainless steel delivery wire. The softness of platinum allows the coil to conform to the often irregular shape of intracranial aneurysms. The coil is used to occlude the aneurysmal sac. To deliver these coils, a specially designed Tracker™ micro-catheter is carefully guided into the aneurysm. The delivery wire /coil combination is then threaded through the micro-catheter and deployed into the aneurysm. (Figure 1) When the coil is properly positioned it is separated from the delivery wire and releasing the coil inside the aneurysm. (Figure 2) Once the aneurysm is occluded, the Tracker™ micro-catheter is slowly withdrawn. (Figure 3) A follow-up benchmark angiogram is performed immediately to assess the effect of the procedure, and subsequent angiogram is performed as required. |
||||||||||||
|
||||||||||||
| Photo of coiled aneurysm, note coils visible inside. | ||||||||||||
| Future Developments in Endovascular Treatment
The future of endovascular treatment for very large inoperable aneurysms may include placing prosthesis such as a stent in the intracranial vessels. A stent may cover the neck of the aneurysm allowing for safe deposition of coils in the aneurysm without any coil mass protruding into the parent artery. |
||||||||||||
|
||||||||||||
| The current treatment of choice for Vein of Galen Malformations is embolization. For other treatment options, see: http://brainavm.oci.utoronto.ca/malformations/treatment_information.htm | ||||||||||||